GM e-log
K Aravind,roll no 55,9th sem.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment.
A 67 year old Male R/O Devarakonda , came to the casualty 5days back with complaints of Shortness of breath since 10 days and pedal & facial edema since 8 days.
History of presenting illness;
Patient was apparently asymptomatic 10 days back , then he developed Shortness of breath which is insidious in onset, gradually progressive in nature, aggravating on exertion and relieved on taking rest, progressed from grade II to grade III- IV (Modified MRC) Orthopnea, Paroxysmal nocturnal dyspnea present.
He also came with complaints of Bilateral pedal edema below knees , facial puffiness and periorbital edema since 8 days , insidious onset, gradually progressive in nature , no diurnal variation, pitting type I. C/o decreased urine output and decreased appetite since 5days.
No C/o chest pain, palpitations, profuse sweating, No c/o fever, cold,nausea,vomiting.
Daily routine:
Waking up at 6: 00 am, breakfast as idli/upma at 8:00 am . He used to have his lunch as rice and curry , sambhar/rasam at 1: 00 pm .He usually haves his dinner as chapati/upma/rice and curry at 8:00pm and goes to bed by 9:00 pm. The patient used to lead a normal life before this 15days
Past history;
: K/c/o asthma since 10yrs -on medication.
K/C/O HTN 6 yrs ago and used medication for 3 yrs and stopped as BP was under control H/O TB 30 yrs ago.
N/K/C/O DM, CAD, CVD, Thyroid, epilepsy .
Family history; N/K/C/O DM, HTN, Asthma, Epilepsy, CAD, CVD, TB, Thyroid.
Personal history;
Mixed diet
decreased appetite.
Sleep adequate
Urinene output decreased .
Bowel movements: Regular.
Addictions: Alcohol occasionally.
Allergies: no known.
General examination;
Patient is drowsy due to sedation, coherent to time , place, person.
Ht: 155cm
Wt: 58 kg
Pallor: present.
Icterus: absent .
Clubbing: absent .
Cyanosis: absent .
Koilonychia: absent .
Lymphadenopathy.absent .
Vitals:
Temp: 98 F
BP: 90/60 mmHg
PR: 102 bpm
RR: 15 cpm
SpO2: 100% at 5 litre O2
GRBS: 126 mg% .
Systemic examination;
RS:
Orthopnea + Paroxysmal nocturnal dyspnoea + wheeze + Central position of trachea NVBS + .
CVS:
S1 S2 heard No murmurs No thrills .
ABDOMEN:
Shape of abdomen: mildly distended No tenderness No palpable mass No bruits Liver and spleen- not palpable Bowel sounds heard .
CNS:
drowsy but arousable no neck stiffness kernig's sign negative cranial nerves: normal motor - intact ,sensory - intact.
Glasgow scale E2V2M2 = 6/15 .
MUSCULOSKELETAL SYSTEM:
normal SKIN: normal ENT: normal TOOTH & ORAL CAVITY: normal .
Physical examination;


Provional diagnosis;
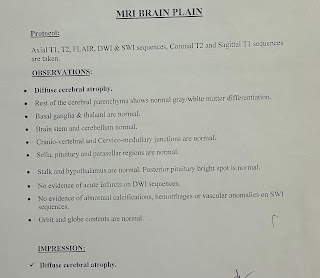
Altered sensorium ? AKI ??
HEART FAILURE(ET 51%)
ANAEMIA.
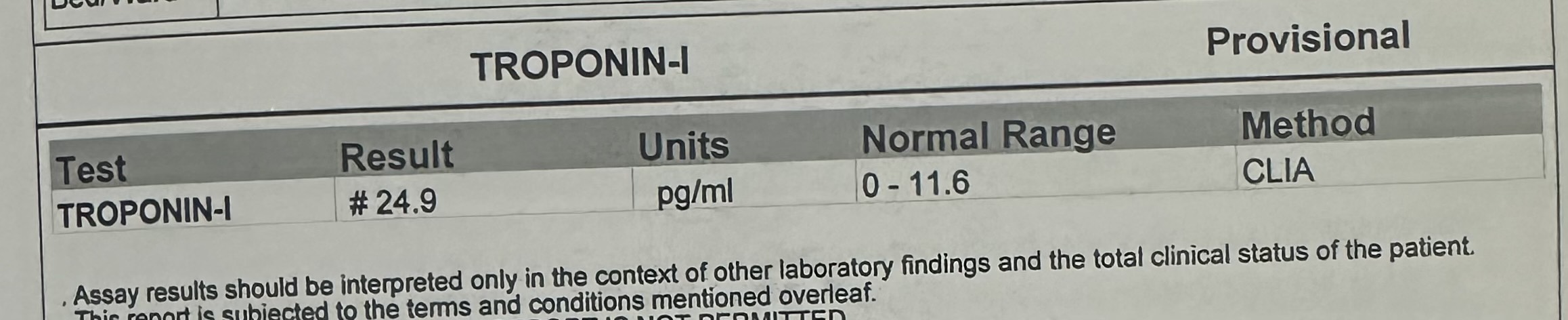
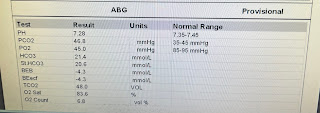
Investigations;
2/12/2023:
























 .
. 
6/12/2023



Comments
Post a Comment